
Course and Survival of COVID-19 Patients with Comorbidities in Relation to the Trace Element Status at Hospital Admission

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessment of Disease Severity
- Class A (mild): no infiltrates on chest X-ray or CT thorax (study 1), or asymptomatic disease severity as assessed by the treating physician (study 2)
- Class B (moderate): fever or history of fever or respiratory symptoms (cough, cough with sputum, wheezing, chest pain, shortness of breath, lower chest wall indrawing) and infiltrates on chest X-ray or CT thorax (study 1), or symptoms of infection, little (<3 L) oxygen requirement and fast discharge (study 2)
- Class C (severe): respiration rate >30/min or SpO2 <93% (rest) or PF-ratio <300 mmHg at any time during hospitalization (study 1), or moderate disease severity with oxygen deficiency (study 2)
- Class D (critical): mechanical ventilation or septic shock or ICU stay at any time during hospitalization (study 1), or severe oxygen deficiency (or intubation), difficult recovery, signs of severe infection (study 2)
- Class E (death): disease severity finally resulting in death (study 1, study 2).
2.3. Analysis of Blood Samples
2.4. Statistical Analysis
3. Results
3.1. Trace Element Status at Hospital Admission
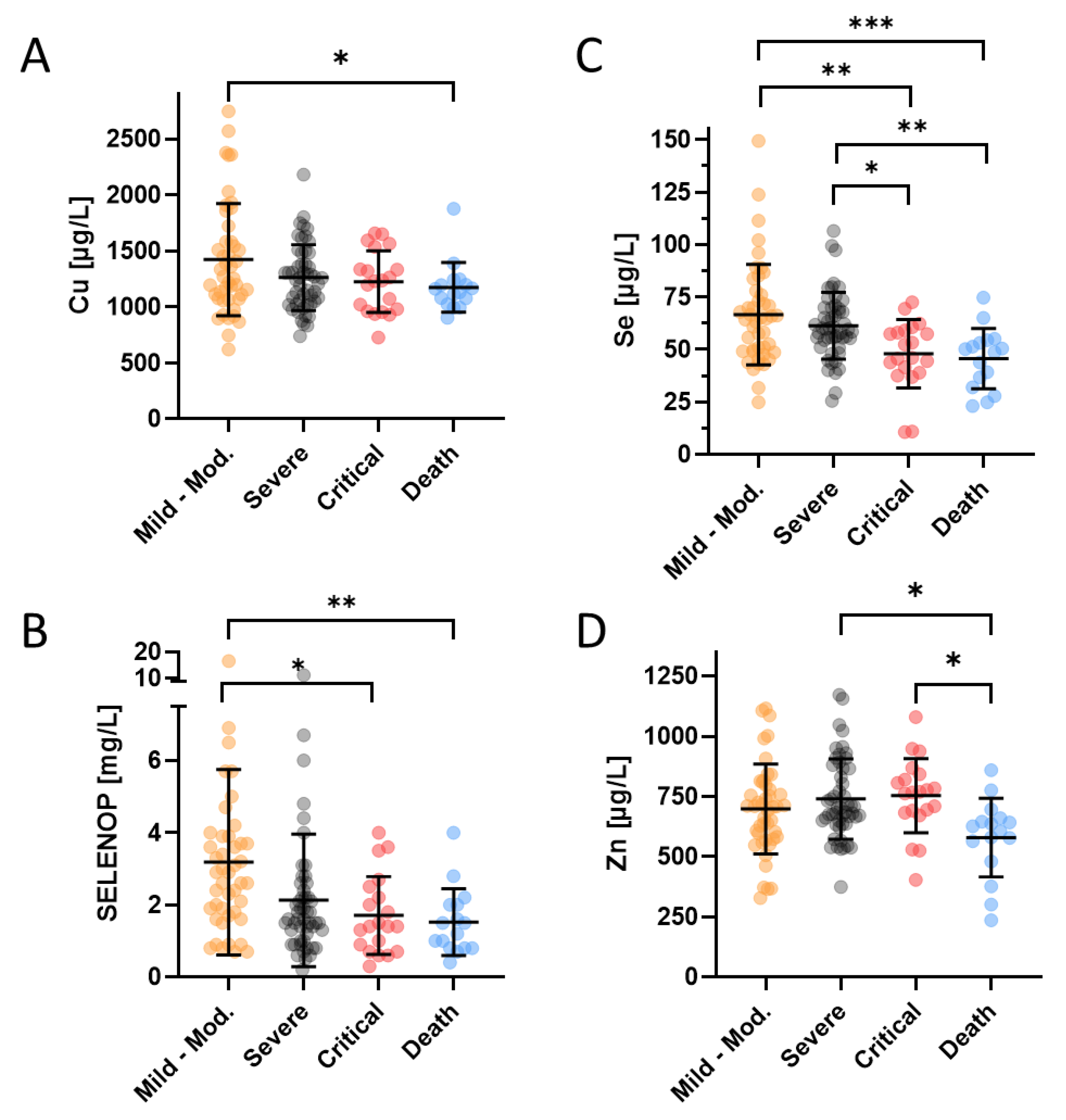
3.2. Relation between Trace Element Status and Disease Severity
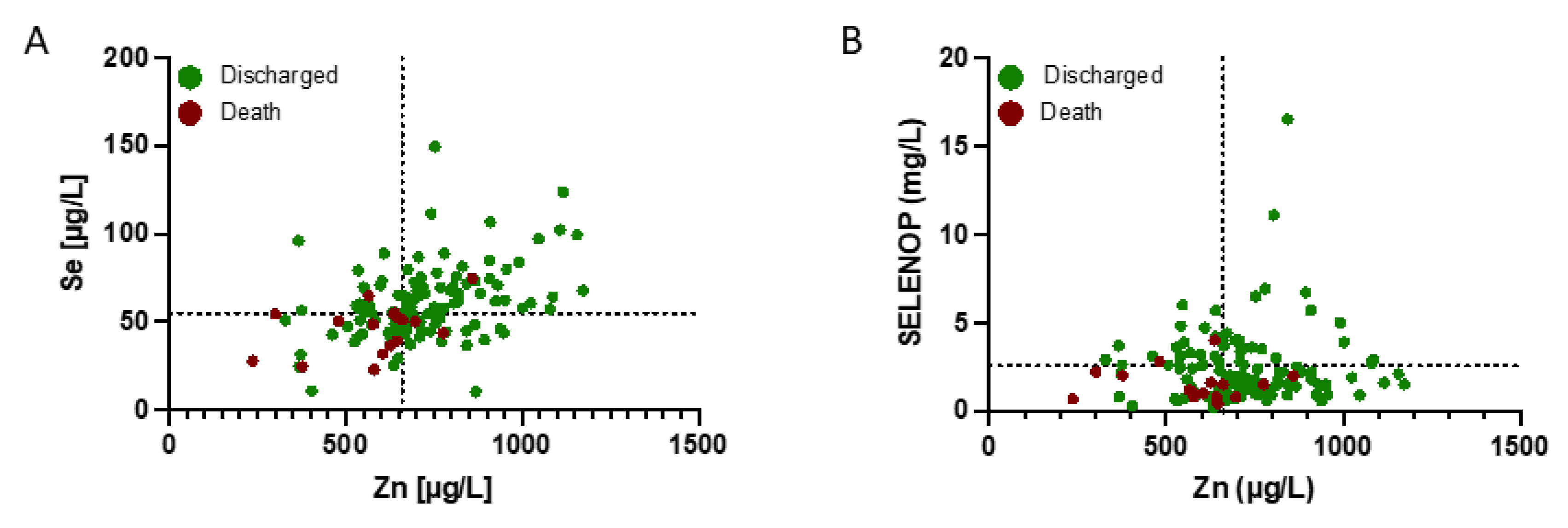
3.3. Clinical Relevance of Se and Zn Deficits for Disease Severity
3.4. Interrelation between Trace Element Status and Mortality in Relation to Comorbidities
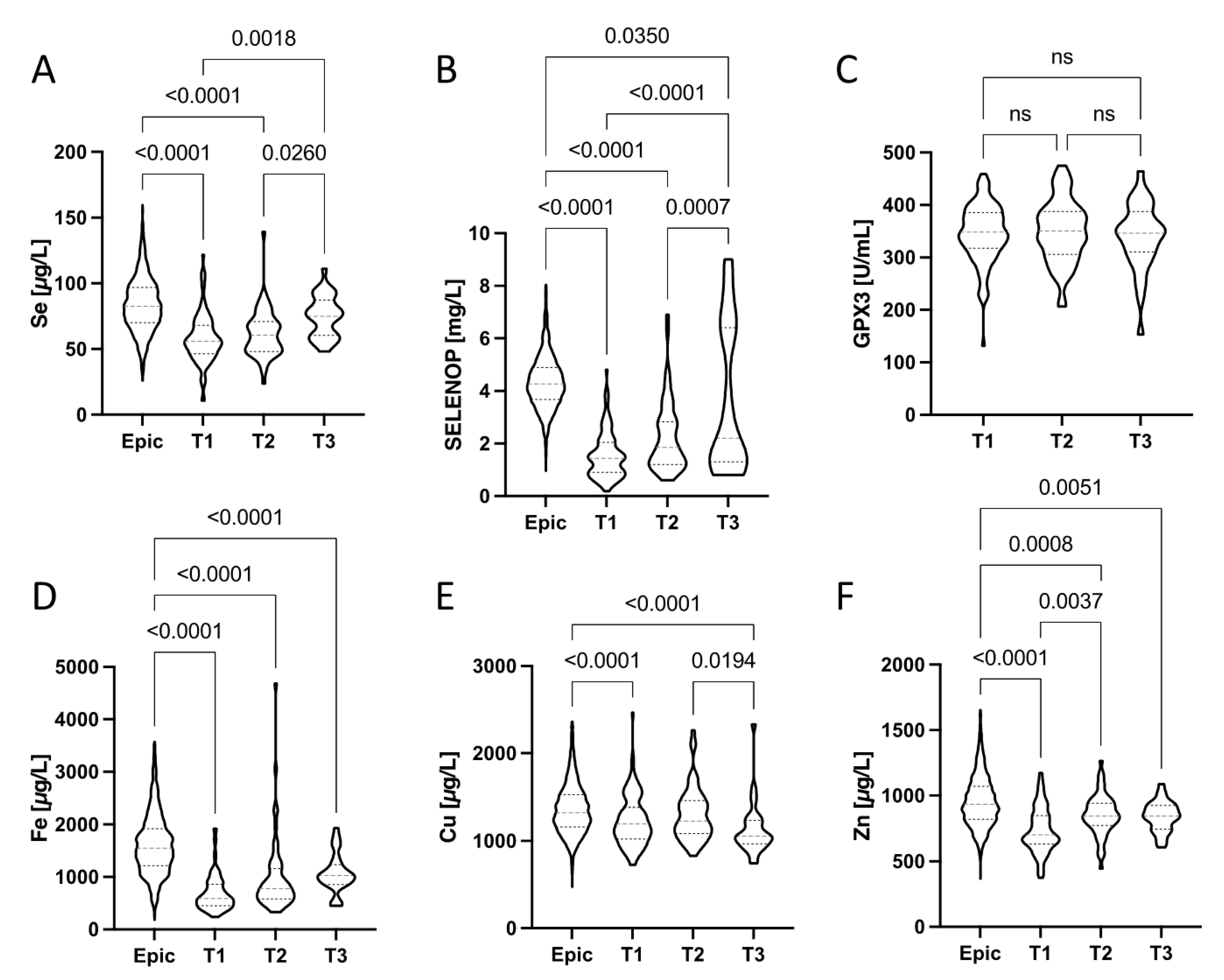
3.5. Trace Element Dynamics from Hospital Admission to Discharge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steinman, J.B.; Lum, F.M.; Ho, P.P.; Kaminski, N.; Steinman, L. Reduced development of COVID-19 in children reveals molecular checkpoints gating pathogenesis illuminating potential therapeutics. Proc. Natl. Acad. Sci. USA 2020, 117, 24620–24626. [Google Scholar] [CrossRef]
- Ng, W.H.; Tipih, T.; Makoah, N.A.; Vermeulen, J.G.; Goedhals, D.; Sempa, J.B.; Burt, F.J.; Taylor, A.; Mahalingam, S. Comorbidities in SARS-CoV-2 Patients: A Systematic Review and Meta-Analysis. mBio 2021, 12, e03647-20. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Santos, A.L.; Sinha, S. Obesity and aging: Molecular mechanisms and therapeutic approaches. Ageing Res. Rev. 2021, 67, 101268. [Google Scholar] [CrossRef]
- Sies, H.; Jones, D.P. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat. Rev. Mol. Cell Biol. 2020, 21, 363–383. [Google Scholar] [CrossRef]
- Lossow, K.; Kopp, J.F.; Schwarz, M.; Finke, H.; Winkelbeiner, N.; Renko, K.; Meci, X.; Ott, C.; Alker, W.; Hackler, J.; et al. Aging affects sex- and organ-specific trace element profiles in mice. Aging 2020, 12, 13762–13790. [Google Scholar] [CrossRef] [PubMed]
- Cabral, M.; Kuxhaus, O.; Eichelmann, F.; Kopp, J.F.; Alker, W.; Hackler, J.; Kipp, A.P.; Schwerdtle, T.; Haase, H.; Schomburg, L.; et al. Trace element profile and incidence of type 2 diabetes, cardiovascular disease and colorectal cancer: Results from the EPIC-Potsdam cohort study. Eur. J. Nutr. 2021, 60, 3267–3278. [Google Scholar] [CrossRef] [PubMed]
- Haase, H.; Schomburg, L. You’d Better Zinc-Trace Element Homeostasis in Infection and Inflammation. Nutrients 2019, 11, 2078. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C.; Bosco, N.; Bourdet-Sicard, R.; Capuron, L.; Delzenne, N.; Dore, J.; Franceschi, C.; Lehtinen, M.J.; Recker, T.; Salvioli, S.; et al. Health relevance of the modification of low grade inflammation in ageing (inflammageing) and the role of nutrition. Ageing Res. Rev. 2017, 40, 95–119. [Google Scholar] [CrossRef] [PubMed]
- Subedi, L.; Tchen, S.; Gaire, B.P.; Hu, B.; Hu, K. Adjunctive Nutraceutical Therapies for COVID-19. Int. J. Mol. Sci. 2021, 22, 1963. [Google Scholar] [CrossRef] [PubMed]
- Bermano, G.; Meplan, C.; Mercer, D.K.; Hesketh, J.E. Selenium and viral infection: Are there lessons for COVID-19? Brit. J. Nutr. 2021, 125, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Gasmi, A.; Tippairote, T.; Mujawdiya, P.K.; Peana, M.; Menzel, A.; Dadar, M.; Benahmed, A.G.; Bjorklund, G. Micronutrients as immunomodulatory tools for COVID-19 management. Clin. Immunol. 2020, 220, 108545. [Google Scholar] [CrossRef]
- Wessels, I.; Rolles, B.; Rink, L. The Potential Impact of Zinc Supplementation on COVID-19 Pathogenesis. Front. Immunol. 2020, 11, 1712. [Google Scholar] [CrossRef] [PubMed]
- Gorji, A.; Khaleghi Ghadiri, M. Potential roles of micronutrient deficiency and immune system dysfunction in the coronavirus disease 2019 (COVID-19) pandemic. Nutrition 2021, 82, 111047. [Google Scholar] [CrossRef]
- Labunskyy, V.M.; Hatfield, D.L.; Gladyshev, V.N. Selenoproteins: Molecular pathways and physiological roles. Physiol. Rev. 2014, 94, 739–777. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, P.R.; Berry, M.J. The influence of selenium on immune responses. Mol. Nutr. Food Res. 2008, 52, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Steinbrenner, H.; Al-Quraishy, S.; Dkhil, M.A.; Wunderlich, F.; Sies, H. Dietary selenium in adjuvant therapy of viral and bacterial infections. Adv. Nutr. 2015, 6, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Wiehe, L.; Cremer, M.; Wisniewska, M.; Becker, N.P.; Rijntjes, E.; Martitz, J.; Hybsier, S.; Renko, K.; Buhrer, C.; Schomburg, L. Selenium status in neonates with connatal infection. Br. J. Nutr. 2016, 116, 504–513. [Google Scholar] [CrossRef] [Green Version]
- Beck, M.A.; Shi, Q.; Morris, V.C.; Levander, O.A. Rapid genomic evolution of a non-virulent coxsackievirus B3 in selenium-deficient mice results in selection of identical virulent isolates. Nat. Med. 1995, 1, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.A.; Nelson, H.K.; Shi, Q.; Van Dael, P.; Schiffrin, E.J.; Blum, S.; Barclay, D.; Levander, O.A. Selenium deficiency increases the pathology of an influenza virus infection. FASEB J. 2001, 15, 1481–1483. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, I.; Zhang, W.; Brighton, L.E.; Carson, J.L.; Styblo, M.; Beck, M.A. Selenium deficiency alters epithelial cell morphology and responses to influenza. Free Radic. Biol. Med. 2007, 42, 1826–1837. [Google Scholar] [CrossRef] [Green Version]
- Levander, O.A. The selenium-coxsackievirus connection: Chronicle of a collaboration. J. Nutr. 2000, 130, 485S–488S. [Google Scholar] [CrossRef] [Green Version]
- Kipp, A.P.; Strohm, D.; Brigelius-Flohe, R.; Schomburg, L.; Bechthold, A.; Leschik-Bonnet, E.; Heseker, H.; German Nutrition, S. Revised reference values for selenium intake. J. Trace Elem. Med. Biol. 2015, 32, 195–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Taylor, E.W.; Bennett, K.; Saad, R.; Rayman, M.P. Association between regional selenium status and reported outcome of COVID-19 cases in China. Am. J. Clin. Nutr. 2020, 111, 1297–1299. [Google Scholar] [CrossRef]
- Moghaddam, A.; Heller, R.A.; Sun, Q.; Seelig, J.; Cherkezov, A.; Seibert, L.; Hackler, J.; Seemann, P.; Diegmann, J.; Pilz, M.; et al. Selenium Deficiency Is Associated with Mortality Risk from COVID-19. Nutrients 2020, 12, 2098. [Google Scholar] [CrossRef] [PubMed]
- Hulisz, D. Efficacy of zinc against common cold viruses: An overview. J. Am. Pharm. Assoc. 2004, 44, 594–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suara, R.O.; Crowe, J.E., Jr. Effect of zinc salts on respiratory syncytial virus replication. Antimicrob. Agents Chemother. 2004, 48, 783–790. [Google Scholar] [CrossRef] [Green Version]
- Femiano, F.; Gombos, F.; Scully, C. Recurrent herpes labialis: A pilot study of the efficacy of zinc therapy. J. Oral Pathol. Med. 2005, 34, 423–425. [Google Scholar] [CrossRef]
- Rolles, B.; Maywald, M.; Rink, L. Influence of zinc deficiency and supplementation on NK cell cytotoxicity. J. Funct. Foods 2018, 48, 322–328. [Google Scholar] [CrossRef]
- Heller, R.A.; Sun, Q.; Hackler, J.; Seelig, J.; Seibert, L.; Cherkezov, A.; Minich, W.B.; Seemann, P.; Diegmann, J.; Pilz, M.; et al. Prediction of survival odds in COVID-19 by zinc, age and selenoprotein P as composite biomarker. Redox Biol. 2021, 38, 101764. [Google Scholar] [CrossRef]
- Vogel-Gonzalez, M.; Tallo-Parra, M.; Herrera-Fernandez, V.; Perez-Vilaro, G.; Chilton, M.; Nogues, X.; Gomez-Zorrilla, S.; Lopez-Montesinos, I.; Arnau-Barres, I.; Sorli-Redo, M.L.; et al. Low Zinc Levels at Admission Associates with Poor Clinical Outcomes in SARS-CoV-2 Infection. Nutrients 2021, 13, 562. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.J.; Fedirko, V.; Jenab, M.; Schomburg, L.; Meplan, C.; Freisling, H.; Bueno-de-Mesquita, H.B.; Hybsier, S.; Becker, N.P.; Czuban, M.; et al. Selenium status is associated with colorectal cancer risk in the European prospective investigation of cancer and nutrition cohort. Int. J. Cancer 2015, 136, 1149–1161. [Google Scholar] [CrossRef]
- Salonen, J.T.; Alfthan, G.; Huttunen, J.K.; Pikkarainen, J.; Puska, P. Association between Cardiovascular Death and Myocardial-Infarction and Serum Selenium in a Matched-Pair Longitudinal-Study. Lancet 1982, 2, 175–179. [Google Scholar] [CrossRef]
- Brodin, O.; Hackler, J.; Misra, S.; Wendt, S.; Sun, Q.; Laaf, E.; Stoppe, C.; Bjornstedt, M.; Schomburg, L. Selenoprotein P as Biomarker of Selenium Status in Clinical Trials with Therapeutic Dosages of Selenite. Nutrients 2020, 12, 1067. [Google Scholar] [CrossRef] [Green Version]
- Monsen, E.R. Dietary reference intakes for the antioxidant nutrients: Vitamin C, vitamin E, selenium, and carotenoids. J. Am. Diet. Assoc. 2000, 100, 637–640. [Google Scholar] [CrossRef]
- Majeed, M.; Nagabhushanam, K.; Gowda, S.; Mundkur, L. An exploratory study of selenium status in healthy individuals and in patients with COVID-19 in a south Indian population: The case for adequate selenium status. Nutrition 2021, 82, 111053. [Google Scholar] [CrossRef] [PubMed]
- Guillin, O.M.; Vindry, C.; Ohlmann, T.; Chavatte, L. Selenium, Selenoproteins and Viral Infection. Nutrients 2019, 11, 2101. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Rose, A.H.; Hoffmann, P.R. The role of selenium in inflammation and immunity: From molecular mechanisms to therapeutic opportunities. Antioxid. Redox Signal. 2012, 16, 705–743. [Google Scholar] [CrossRef] [Green Version]
- Renko, K.; Hofmann, P.J.; Stoedter, M.; Hollenbach, B.; Behrends, T.; Kohrle, J.; Schweizer, U.; Schomburg, L. Down-regulation of the hepatic selenoprotein biosynthesis machinery impairs selenium metabolism during the acute phase response in mice. FASEB J. 2009, 23, 1758–1765. [Google Scholar] [CrossRef]
- Stoedter, M.; Renko, K.; Hog, A.; Schomburg, L. Selenium controls the sex-specific immune response and selenoprotein expression during the acute-phase response in mice. Biochem. J. 2010, 429, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Maehira, F.; Luyo, G.A.; Miyagi, I.; Oshiro, M.; Yamane, N.; Kuba, M.; Nakazato, Y. Alterations of serum selenium concentrations in the acute phase of pathological conditions. Clin. Chim. Acta 2002, 316, 137–146. [Google Scholar] [CrossRef]
- Sherlock, L.G.; Sjostrom, K.; Sian, L.; Delaney, C.; Tipple, T.E.; Krebs, N.F.; Nozik-Grayck, E.; Wright, C.J. Hepatic-Specific Decrease in the Expression of Selenoenzymes and Factors Essential for Selenium Processing After Endotoxemia. Front. Immunol. 2020, 11, 595282. [Google Scholar] [CrossRef]
- Forceville, X.; Vitoux, D.; Gauzit, R.; Combes, A.; Lahilaire, P.; Chappuis, P. Selenium, systemic immune response syndrome, sepsis, and outcome in critically ill patients. Crit. Care Med. 1998, 26, 1536–1544. [Google Scholar] [CrossRef]
- Berger, M.M.; Manzanares, W. Micronutrients early in critical illness, selective or generous, enteral or intravenous? Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 165–175. [Google Scholar] [CrossRef]
- Stone, C.A.; Kawai, K.; Kupka, R.; Fawzi, W.W. Role of selenium in HIV infection. Nutr. Rev. 2010, 68, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.A.; Handy, J.; Levander, O.A. Host nutritional status: The neglected virulence factor. Trends Microbiol. 2004, 12, 417–423. [Google Scholar] [CrossRef]
- Braunstein, M.; Kusmenkov, T.; Zuck, C.; Angstwurm, M.; Becker, N.P.; Bocker, W.; Schomburg, L.; Bogner-Flatz, V. Selenium and Selenoprotein P Deficiency Correlates with Complications and Adverse Outcome After Major Trauma. Shock 2020, 53, 63–70. [Google Scholar] [CrossRef]
- Alexander, J.; Tinkov, A.; Strand, T.A.; Alehagen, U.; Skalny, A.; Aaseth, J. Early Nutritional Interventions with Zinc, Selenium and Vitamin D for Raising Anti-Viral Resistance Against Progressive COVID-19. Nutrients 2020, 12, 2358. [Google Scholar] [CrossRef] [PubMed]
- Samad, N.; Sodunke, T.E.; Abubakar, A.R.; Jahan, I.; Sharma, P.; Islam, S.; Dutta, S.; Haque, M. The Implications of Zinc Therapy in Combating the COVID-19 Global Pandemic. J. Inflamm. Res. 2021, 14, 527–550. [Google Scholar] [CrossRef] [PubMed]
- Jothimani, D.; Kailasam, E.; Danielraj, S.; Nallathambi, B.; Ramachandran, H.; Sekar, P.; Manoharan, S.; Ramani, V.; Narasimhan, G.; Kaliamoorthy, I.; et al. COVID-19: Poor outcomes in patients with zinc deficiency. Int. J. Infect. Dis. 2020, 100, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.D. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur. J. Clin. Nutr. 2004, 58, 391–402. [Google Scholar] [CrossRef] [Green Version]
- Schomburg, L. The other view: The trace element selenium as a micronutrient in thyroid disease, diabetes, and beyond. Hormones 2020, 19, 15–24. [Google Scholar] [CrossRef]
- Alfthan, G.; Eurola, M.; Ekholm, P.; Venalainen, E.R.; Root, T.; Korkalainen, K.; Hartikainen, H.; Salminen, P.; Hietaniemi, V.; Aspila, P.; et al. Effects of nationwide addition of selenium to fertilizers on foods, and animal and human health in Finland: From deficiency to optimal selenium status of the population. J. Trace Elem. Med. Biol. 2015, 31, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Dettorre, G.M.; Patel, M.; Gennari, A.; Pentheroudakis, G.; Romano, E.; Cortellini, A.; Pinato, D.J. The systemic pro-inflammatory response: Targeting the dangerous liaison between COVID-19 and cancer. ESMO Open 2021, 6, 100123. [Google Scholar] [CrossRef] [PubMed]
- Buicu, A.L.; Cernea, S.; Benedek, I.; Buicu, C.F.; Benedek, T. Systemic Inflammation and COVID-19 Mortality in Patients with Major Noncommunicable Diseases: Chronic Coronary Syndromes, Diabetes and Obesity. J. Clin. Med. 2021, 10, 1545. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cancer | Diabetes | Obesity | Cardiac Disease | BMI | Disease Severity A/B/C/D/E * | ||
|---|---|---|---|---|---|---|---|
| n | n | n | n | n | Mean ± SD | n | |
| All patients | 79 | 13 | 24 | 22 | 22 | 28.5 ± 5.2 | 2/8/39/20/10 |
| Male Female | 55 24 | 9 4 | 15 9 | 16 6 | 19 3 | 28.9 ± 5.2 27.0 ± 5.1 | 1/7/24/15/8 1/1/15/5/2 |
| Malignant neoplasm+ | 13 | 13 | 2 | 3 | 5 | 27.6 ± 4.5 | 0/1/5/4/3 |
| Malignant neoplasm− | 66 | 0 | 22 | 19 | 17 | 28.7 ± 5.4 | 2/7/34/16/7 |
| Diabetes+ | 24 | 2 | 24 | 14 | 9 | 30.2 ± 5.9 | 0/2/11/7/4 |
| Diabetes− | 55 | 11 | 0 | 8 | 13 | 27.7 ± 4.8 | 2/6/28/13/6 |
| Obesity+ | 22 | 3 | 14 | 22 | 7 | 34.5 ± 4.1 | 0/3/8/9/2 |
| Obesity− | 48 | 8 | 9 | 0 | 15 | 25.8 ± 3.3 | 1/4/26/10/7 |
| Chronic cardiac disease+ | 22 | 5 | 9 | 7 | 22 | 27.7 ± 5.5 | 2/2/7/6/5 |
| Chronic cardiac disease− | 57 | 8 | 15 | 15 | 0 | 28.8 ± 5.1 | 0/6/32/14/5 |
| Below 65 years | 46 | 7 | 11 | 14 | 7 | 29.9 ± 7.4 | 0/7/24/13/2 |
| 65–80 years | 26 | 4 | 8 | 5 | 9 | 26.6 ± 4.7 | 1/1/15/6/3 |
| Above 80 years | 7 | 2 | 5 | 3 | 6 | 26.8 ± 3.0 | 1/0/0/1/5 |
| Se [µg L−1] | Zn [µg L−1] | SELENOP [mg L−1] | Cu [µg L−1] | Fe [µg L−1] | GPX3 [U L−1] | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| All patients of study 1 | 79 | 56.6 | 16.9 | 735 | 166 | 1.6 | 0.9 | 1168 | 229 | 689 | 331 | 349 | 51 |
| Male | 55 | 57.6 | 16.1 | 729 | 164 | 1.6 | 1.0 | 1125 | 190 | 737 | 352 | 351 | 54 |
| Female | 24 | 54.2 | 18.7 | 748 | 173 | 1.5 | 0.9 | 1268 | 279 | 578 | 252 | 346 | 45 |
| p-value | 0.405 | 0.645 | 0.924 | 0.018 | 0.038 | 0.726 | |||||||
| Until 65 years | 49 | 58.2 | 19.1 | 747 | 182 | 1.5 | 0.8 | 1170 | 245 | 703 | 367 | 360 | 50 |
| Above 65 years | 30 | 53.9 | 12.4 | 715 | 135 | 1.7 | 1.1 | 1164 | 205 | 666 | 269 | 332 | 48 |
| p-value | 0.275 | 0.409 | 0.808 | 0.856 | 0.840 | 0.017 | |||||||
| Malignant neoplasm+ | 13 | 50.2 | 9.1 | 623 | 113 | 1.1 | 0.6 | 1100 | 186 | 560 | 187 | 336 | 52 |
| Malignant neoplasm− | 66 | 57.8 | 17.9 | 757 | 166 | 1.7 | 0.9 | 1181 | 235 | 714 | 348 | 352 | 51 |
| p-value | 0.140 | 0.007 | 0.022 | 0.200 | 0.202 | 0.315 | |||||||
| Diabetes+ | 24 | 52.2 | 15.5 | 767 | 171 | 1.4 | 0.8 | 1156 | 191 | 634 | 259 | 340 | 42 |
| Diabetes− | 55 | 58.5 | 17.3 | 720 | 163 | 1.6 | 1.0 | 1173 | 245 | 713 | 358 | 353 | 54 |
| p-value | 0.128 | 0.254 | 0.343 | 0.798 | 0.449 | 0.279 | |||||||
| Obesity+ | 22 | 52.2 | 16.7 | 7701 | 167 | 1.5 | 1.0 | 1199 | 208 | 584 | 209 | 342 | 44 |
| Obesity− | 48 | 58.2 | 16.9 | 754 | 165 | 1.6 | 0.9 | 1169 | 242 | 741 | 351 | 352 | 52 |
| p-value | 0.173 | 0.220 | 0.383 | 0.433 | 0.077 | 0.425 | |||||||
| Chronic cardiac disease+ | 22 | 55.5 | 15.0 | 737 | 127 | 1.3 | 0.9 | 1137 | 217 | 722 | 365 | 322 | 49 |
| Chronic cardiac disease− | 57 | 57.0 | 17.7 | 734 | 180 | 1.7 | 0.9 | 1180 | 234 | 676 | 320 | 356 | 51 |
| p-value | 0.731 | 0.928 | 0.134 | 0.347 | 0.687 | 0.064 | |||||||
| Mortality [%] | Full Group | Zn Deficient | Zn Sufficient | p-Value | Se Deficient | Se Sufficient | p-Value |
|---|---|---|---|---|---|---|---|
| Total group | 13.7 (10/73) | 29.2 (7/24) | 6.1 (3/49) | 0.009 | 29.0 (9/31) | 2.4 (1/42) | <0.001 |
| Until 65 years | 4.4 (2/45) | 7.7 (1/13) | 3.1 (1/32) | 0.164 | 6.3 (1/16) | 3.4 (1/29) | 0.328 |
| Above 65 years | 28.6 (8/28) | 54.5 (6/11) | 13.3 (2/17) | 0.045 | 53.3 (8/15) | 0.0 (0/13) | <0.001 |
| p-value | 0.004 | 0.009 | 0.244 | 0.002 | 0.386 | ||
| Diabetes+ | 16.7 (4/24) | 50.0 (3/6) | 5.6 (1/18) | 0.018 | 30.8 (4/13) | 0.0 (0/11) | 0.018 |
| Diabetes− | 12.2 (6/49) | 22.2 (4/18) | 6.5 (2/31) | 0.111 | 27.8 (5/18) | 3.2 (1/31) | 0.012 |
| p-value | 0.611 | 0.208 | 0.899 | 0.857 | 0.433 | ||
| Malignant neoplasm+ | 25.0 (3/12) | 28.6 (2/7) | 20.0 (1/5) | 0.733 | 42.9 (3/7) | 0.0 (0/5) | 0.047 |
| Malignant neoplasm− | 11.4 (7/61) | 29.4 (5/17) | 4.5 (2/44) | 0.010 | 25.0 (6/24) | 2.7 (1/37) | 0.007 |
| p-value | 0.245 | 0.967 | 0.255 | 0.612 | 0.372 | ||
| Cardiac disease+ | 25.0 (5/20) | 42.9 (3/7) | 15.4 (2/13) | 0.183 | 41.7 (5/12) | 0.0 (0/8) | 0.013 |
| Cardiac disease− | 9.4 (5/53) | 23.5 (4/17) | 2.8 (1/36) | 0.020 | 21.1 4/19 | 2.9 (1/34) | 0.033 |
| p-value | 0.100 | 0.353 | 0.132 | 0.222 | 0.513 | ||
| Obesity+ | 11.1 (2/18) | 33.3 (2/6) | 0.0 (0/12) | 0.027 | 22.2 (2/9) | 0.0 (0/9) | 0.082 |
| Obesity− | 14.9 (7/47) | 26.7 (4/15) | 9.4 (3/32) | 0.134 | 31.6 (6/19) | 3.6 (1/28) | 0.007 |
| p-value | 0.687 | 0.762 | 0.158 | 0.604 | 0.452 |
| Age Group | TERS | Number (% of Total) | Non-Surviving (Class E) * | Critical (Class D) * | Severe (Class C) * | Mild to Moderate (Class A + B) * |
|---|---|---|---|---|---|---|
| entire cohort | 0 | 17 (13%) | 8 (50/47) | 2 (10/12) | 3 (6/18) | 4 (9/24) |
| 1 | 40 (30%) | 7 (44/18) | 8 (40/20) | 13 (25/33) | 12 (27/30) | |
| 2 | 45 (34%) | 0 (0/0) | 6 (30/13) | 25 (49/56) | 14 (31/31) | |
| 3 | 30 (23%) | 1 (6/3) | 4 (20/13) | 10 (20/33) | 15 (33/50) | |
| above 65 y | 0 | 9 (14%) | 7 (58/78) | 0 (0/0) | 1 (5/11) | 1 (5/11) |
| 1 | 19 (32%) | 5 (42/26) | 4 (44/21) | 7 (37/37) | 3 (16/16) | |
| 2 | 15 (26%) | 0 (0/0) | 1 (11/7) | 7 (37/47) | 7 (37/47) | |
| 3 | 16 (28%) | 0 (0/0) | 4 (44/25) | 4 (21/25) | 8 (42/50) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du Laing, G.; Petrovic, M.; Lachat, C.; De Boevre, M.; Klingenberg, G.J.; Sun, Q.; De Saeger, S.; De Clercq, J.; Ide, L.; Vandekerckhove, L.; et al. Course and Survival of COVID-19 Patients with Comorbidities in Relation to the Trace Element Status at Hospital Admission. Nutrients 2021, 13, 3304. https://doi.org/10.3390/nu13103304
Du Laing G, Petrovic M, Lachat C, De Boevre M, Klingenberg GJ, Sun Q, De Saeger S, De Clercq J, Ide L, Vandekerckhove L, et al. Course and Survival of COVID-19 Patients with Comorbidities in Relation to the Trace Element Status at Hospital Admission. Nutrients. 2021; 13(10):3304. https://doi.org/10.3390/nu13103304
Chicago/Turabian StyleDu Laing, Gijs, Mirko Petrovic, Carl Lachat, Marthe De Boevre, Georg J. Klingenberg, Qian Sun, Sarah De Saeger, Jozefien De Clercq, Louis Ide, Linos Vandekerckhove, and et al. 2021. "Course and Survival of COVID-19 Patients with Comorbidities in Relation to the Trace Element Status at Hospital Admission" Nutrients 13, no. 10: 3304. https://doi.org/10.3390/nu13103304